
The doctors at Orthodontists Associates of WNY has created The Complete Orthodontic Care Guide to help parents and patients of orthodontics understand the types treatments.
Download Our Free Orthodontic Care Guide
 As a parent, you are responsible for the health and well-being of your child(ren). That is no easy task! Ensuring your children have sound oral health can be a challenge if your kids, like so many others, are afraid of dentists. If you have ever had trouble cajoling your child into going to the dentist, this eBook is for you. In the following sections, you will find:
As a parent, you are responsible for the health and well-being of your child(ren). That is no easy task! Ensuring your children have sound oral health can be a challenge if your kids, like so many others, are afraid of dentists. If you have ever had trouble cajoling your child into going to the dentist, this eBook is for you. In the following sections, you will find:
- answers to your questions as well as your child’s
- treatment-specific information for those of your kids undergoing orthodontic treatment
- expert orthodontic advice on what signs you should look out for in your child
- how to decide if your child requires orthodontic care
- information about any orthodontic appliances your child may be using
This comprehensive guide covers every phase of the patient’s journey as well as their parents’. This guide will help you through the entire process, from before you decide seek treatment to after it is complete. While the subjects covered hereafter pertain more specifically to children than to adults, adult patients may also seek orthodontic care and treatment.
The field of orthodontics and dentofacial orthopedics is a specialty within dentistry. This specialty deals with a variety of ways to treat malocclusions. Some patients’ teeth don’t fit together properly. Some others have jaws that don’t fit together. Therefore, our job as orthodontists is to correct these problems. The practice of orthodontics is aimed at correcting malocclusions or misaligned bites. Because each case is unique, an orthodontist usually tailors a treatment to the individualized needs of each child.
When Should Children Start Orthodontic Treatment?
There is no determined age for children to begin orthodontic treatment. However, the American Association of Orthodontists recommends a first screening at age seven. Early treatment allows your orthodontist to
- correct and guide the development of your child’s jaw
- create more space for crowded teeth
- avoid the need for extractions later in life
- correct thumb sucking
- minor speech problems
Parents are encouraged to keep an eye out for certain issues such as crowded or misplaced teeth, difficulty chewing or biting, mouth-breathing, thumb-sucking, or popping jaws. If you notice these issues, it is likely that your child needs to see an orthodontist.
Orthodontics For Teens
Braces are no longer as scary as many adolescents might imagine. Braces today come in a variety of styles, materials and colors making life with braces easier, more comfortable and even stylish. Patients can now choose from different treatment options like traditional metal, ceramic and invisible braces. Treatment times do vary, however. Your body’s response time and how much work is required of the orthodontist are two factors responsible in determining treatment time. Regardless of the type of braces you choose, it is important that you avoid sticky, hard or chewy foods. They may damage your braces and prolong your treatment time.
What Orthodontic Treatments Do We Offer?
The field of orthodontics provides for a variety of methods of treatment. Broadly, these are early orthodontic treatment, dentofacial orthopedics, surgical orthodontics and craniofacial orthodontics. An orthodontist will typically select one or a combination of these to treat patients.
 Early Orthodontic Treatment
Early Orthodontic Treatment
There was a time when most parents didn’t begin to think about the need for orthodontic treatment for their children until the teenage years. Now, parents, dentists and orthodontists alike look toward treating children that haven’t quite hit their teen years.
What Are The Benefits of Early Orthodontic Treatment?
In the past, the trend for orthodontic treatment was to wait until most or all of a child’s permanent teeth had come in. However, most orthodontic problems are much easier to correct sooner rather than later. This is why professionals recommend and insist upon early orthodontic treatment.
Certain orthodontic conditions can be treated as early as 7 or 8 years old. Although they may not be able to be totally corrected at that time, early orthodontic treatment can drastically reduce the amount of treatment that a child needs to undergo during their teen years.
What Are The Most Common Early Orthodontic Treatments?
There are several conditions that can benefit from early orthodontic treatments.
Early or late loss of baby teeth
Children usually lose their baby teeth are in the same order in which the teeth came in for the child. If a patient does not lose baby teeth during the normal time frame or in the right order, there are several issues that can require orthodontic intervention. Crowding of teeth may occur if the baby teeth are lost too soon. If baby teeth fall out too late, the permanent teeth may come in crowded and also be crooked. If a permanent tooth comes in before a baby tooth is lost, it can create crowding. Although crowding isn’t an emergency, it is something that can affect the smile or bite of a child. If a child loses a tooth due to trauma or decay, early orthodontic treatment can include using a spacer to make sure that the permanent tooth comes in correctly.
Orthodontic issues caused by thumb sucking
Prolonged thumb sucking can cause an open bite. An open bite is a term used to describe when the upper and lower teeth are unable to make physical contact with each other. Sometimes an open bite corrects itself, but many times it can only be corrected with orthodontic care. In severe cases, surgery may be required to correct the open bite.
Overbites and underbites
An overbite occurs when the upper jaw is longer than the lower jaw. An underbite occurs when the lower jaw is longer than the upper jaw. Overbites and underbites don’t always cause problems. Yet, even if your child doesn’t suffer from a speech impediment or sinus problems, they may be subject to teasing from other children. Early orthodontic treatment involves taking x-rays and a mold to determine the cause of the misplaced bite. Then, treatment is customized for each child.
Crossbite
A crossbite can be either anterior or posterior. Essentially, it means that when your child bites down, their teeth don’t line up properly. A crossbite can cause dental problems and problems for your child’s self-esteem. It’s possible that an untreated crossbite can cause your child’s face to develop in an asymmetrical fashion. It can also cause gum disease and chronic pain in the jaw, neck and shoulders. A crossbite can be corrected with early orthodontic treatment and can save your child from a life full of chronic pain and low self-esteem.
What Are The Stages Of Early Orthodontic Treatment?
Early orthodontic treatment is usually done in stages. These stages are referred to as Phase I and Phase II. In Phase I, treatment focuses on correcting your child’s bite and teaching your child good oral hygiene. Preventing or lessening a dental issue helps guide the development of the child’s jaw, guides permanent teeth into their proper place, and could also provide a positive boost to your child’s self-esteem. Phase I is all about beginning the corrections that need to occur to help minimize the risk of lifelong dental issues.
Phase II occurs a little bit later into the early orthodontic treatment. This involves the use of braces. The purpose of braces is to help guide your child’s teeth into the proper position and stabilize them. Phase II often doesn’t begin until the child is between 11 and 15 years of age. By this time, their permanent teeth have come in. One of the benefits of waiting until this age for braces is that orthodontists are able to work with the child’s bite and teeth placement during the time they are most likely to grow. This can actually help lessen the amount of time that the child needs to have braces.
How Do I Know If My Child Would Benefit From Early Orthodontic Treatment?
So, just how do you know if your child would benefit from early orthodontic treatment? As a parent, you may see some indications in the way that your child’s smile looks or if they’re complaining of pain in their jaw. Ultimately, the best way to know if your child would benefit from early orthodontic treatment is to take your child to a dental professional. Dentists can take an x-ray and examine your child’s oral health. They can also refer you to an orthodontist who specializes in early treatment. The orthodontist can examine your child and make the determination of whether your child would benefit from early treatment. Not all children need early treatment. This is why it is important to seek out the expert advice of an orthodontist who specializes in treating children.
How To Choose The Right Orthodontist
Choosing the right orthodontist can be daunting. You should always do your homework and make sure they have a great track record. It’s important to choose an orthodontist with experience in early treatment in order to ensure that your child’s assessment and potential treatment is the best it can possibly be.
 What Is Dentofacial Orthopedics?
What Is Dentofacial Orthopedics?
Dentofacial orthopedics is a specialized form of dental care for children and adolescents. The purpose of dentofacial orthopedics is to help guide the growth and development of the face. As you may know, orthopedics is a term that is commonly used to refer to a doctor who specializes in bone health. If you have ever broken a bone, you likely met with an orthopedist. Let’s break down the term “dentofacial orthopedics” so it is clearer. The term “dentofacial” refers specifically to matters of the teeth and the face. The word “orthopedics” has to do with bone health. Therefore, a professional who practices dentofacial orthopedics provides specialized services in matters of the growth and development of the bones in the face as they relate to dental issues.
Why is Dentofacial Orthopedics Used Primarily In Young People?
Dentofacial orthopedics is a common form of treatment for both young people and adults. However, dentofacial orthopedic treatment is usually more tolerable for younger patients. In children and adolescents, the purpose of dentofacial orthopedics is to help guide the growth of the bones. This is easier in children and adolescents because their bones have not yet finished growing.
Adult patients also benefit from dentofacial orthopedic treatment. However, it is important to note that the bones in the face of an adult have finished growing. This is why adults undergoing dentofacial orthopedics will often require surgery during their treatment. This is because it is much more difficult to adjust the bite and move the teeth to the right places in adults.
What Are The Phases Of Dentofacial Orthopedics?
Dentofacial orthopedic treatment occurs in phases with children and adolescents. However, before any work is done, your child will first be examined by a dental professional. This professional will assess your child’s bite and teeth to determine if your child will benefit from dentofacial orthopedics.
Dentofacial orthopedics usually occurs in two phases. The first phase happens if your child has not lost all of their baby teeth. Phase I typically begins when a child is 7-8 years old. Treatment for Phase I focuses on guiding the proper growth of the bones in either jaw. Doing so helps shorten the length of treatment during phase II.
Phase II treatment in dentofacial orthopedics involves the traditional use of braces. Braces are used to align and straighten the teeth. There is a large variety of braces that patients may chose from during this phase of treatment.
What Conditions Are Treated With Dentofacial Orthopedics?
Dentofacial orthopedics is used as a corrective method for misaligned bites. The scientific term for it is “malocclusion”. Simply put, it means that the bite of the patient is misaligned in some form. The degree of this misalignment ranges from minor to severe.
Patients with an overbite – a malocclusion – stand to benefit greatly from dentofacial orthopedics. An overbite is when the upper jaw is longer than the lower jaw. An overbite often tends to result in the overcrowding of teeth. Dentofacial orthopedic appliances are used to correct overbites. Treatment generally lasts between 6-12 months, provided it commences while the patient is between 8-10 years of age. Overbites usually do not cause much of a problem. However, there are some cases where the overbite is more severe. The most common accompanying issue with a severe overbite is a speech impediment. Unfortunately, children often become victims of bullying and teasing at school because of severe malocclusions.
Another malocclusion is an underbite. This occurs when the lower jaw is longer than the upper jaw. Left untreated, it can develop into TMJ disorders. The misalignment causes increased friction. Therefore, your child’s tooth enamel wears down faster. As with overbites, treatment lasts between 6-12 months provided the patient is 8-10 years old.
A crossbite occurs when one jaw is narrower than the other. A crossbite can be either unilateral or bilateral. Furthermore, depending on which jaw is the narrower, your child could have an anterior or a posterior crossbite. Left untreated, a crossbite can lead to gum disease and tooth loss. Moreover, because a crossbite creates an uneven bite, your child’s face could develop asymmetrically. In spite of the serious consequences associated with untreated crossbites, the matter can interestingly take as little as 30 days to treat.
Download Our Free Orthodontic Care Guide
Is Dentofacial Orthopedic Treatment Painful?
Ultimately, the severity of the oral condition is what determines the extent of pain and discomfort a patient might expect. However, most patients report that the discomfort is mild. Often, an over-the counter anti-inflammatory medication tends to suffice. Other patients report feeling more pressure in certain parts of their jaw or mouth while they are wearing the prescribed facial appliances. Conversely, certain other dentofacial orthopedic treatments are virtually painless.
If you or your child undergo dentofacial orthopedic treatment, speak with your dental health provider. They will tell you what to expect and how to manage pain or discomfort.
Better Self-Esteem And Better Dental Health
Several people tend to seek dentofacial orthopedic treatment for cosmetic purposes. While that is not our primary focus, patients report that treatment helped increase self-esteem and boost confidence. When misaligned bites go untreated, they may develop into lifelong issues. Some of these are tooth decay, enamel loss, gum disease, tooth loss, TMJ, and recurrent headaches. Moreover, individuals uncomfortable with their appearances may suffer from low self-esteem. Children with dental problems often face bullying at the hands of their peers. Dentofacial orthopedics corrects dental health problems whilst bolstering patients’ self-esteem. Investing in dentofacial orthopedic treatment promotes the future health of patients.
 What Is Surgical Orthodontics?
What Is Surgical Orthodontics?
Surgical orthodontics is a type of specialized dental treatment. It is performed by orthodontists and not traditional dental practitioners. The purpose of surgical orthodontics is to diagnose and correct several types of conditions. Some conditions may be as simple as something known as a bad bite. Other conditions may be more serious and your orthodontist may need to partner with an oral or maxillofacial surgeon.
Common treatments that fall under the umbrella of surgical orthodontics include mandibular advancement, mandibular setback, maxillary advancement, maxillary setback, correction of an open bite, correction of a gummy smile, and chin advancement. Of course, that’s not a complete list of treatments that fall under surgical orthodontics.
Am I A Candidate for Surgical Orthodontics?
Usually, surgical orthodontics don’t begin until between the ages of 16 and 18 years old. Of course, it can also be used for older patients. In girls, the jaw usually stops growing around the time that they are 16 years old. In boys, the jaw doesn’t stop growing until they are around 18 years old. The reason why surgical orthodontic treatment doesn’t occur until this age (or later) is because the goal of the surgery is to align the jaws (which create the bite of the patient). If the jaws are still growing, performing surgical orthodontics would not be able to achieve its stated purpose. After surgery, the jaw would still grow and that could cause a misalignment.
Surgical orthodontics is only used when braces and other dental appliances cannot completely fix the bite on their own. Your orthodontist will let you know if you are a candidate for surgical orthodontics.
Why Might Surgical Orthodontics Be Required?
- Mandibular advancement. This means that you have an under-developed lower jaw. This creates an overbite. In surgical orthodontics, incisions are made so that the jaws can be properly aligned.
- Mandibular setback. Mandibular setback means that your upper-jaw is under-developed. This causes you to have an underbite. Much like with a mandibular advancement, the goal of surgery is to align the jaws to correct your bite.
- Maxillary advancement. Maxillary advancement creates a form of underbite that’s known as a crossbite. The incisions for this condition is usually made in the mouth on the upper jaw near where it would line up with the eye sockets.
- Maxillary setback. Maxillary setback creates a form of overbite that’s known as an overjet. This surgery actually isn’t as common as a mandibular setback although they may seem similar to you as a patient. With maxillary setback, overjet is caused by the fact that the lower jaw simply did not grow enough.
- An openbite is known as maxillary impaction. The objective of surgical orthodontics is to correct the space between the front and back teeth when you bite down. Bone from the upper jaw is removed and placed higher in order to help correct the problem. The lower jaw is repositioned as well.
- Gummy smile. A gummy smile means that when you smile there is a large amount of gum that is displayed when compared with others. A portion of the upper jaw bone may be moved and placed higher in order to pull the gums up and lessen the amount of gum that is displayed when you smile.
- Chin advancement. Chin advancement is used for patients who have a weak jaw line. This can be used to do more than strengthen the jaw line. It can also be used to help fix the bite of the patient. Depending on the initial diagnosis, you may not need further orthodontic treatment after this procedure.
How Does Surgical Orthodontics Work?
The first step in surgical orthodontics is to develop a treatment plan with your orthodontist. The orthodontist and your oral surgeon will work together to develop a plan that will best suit your specific needs. This could include setting up plaster or 3D models of your mouth, jaw, and entire face. Other specialists, including an ENT and speech therapist, may also be part of the treatment plan depending on the severity of the dental condition being treated.
Usually, the second part of treatment is the use of braces. The use of braces is an important component in your surgical orthodontic treatment. It helps create reference points in order for the oral surgeons to be able to do their job.
Next, one or more surgeries will take place in order to correct the dental issue or issues being treated. The number of surgeries you’ll need will largely depend on the severity of your dental problem. Generally, children require fewer surgeries than adults. This is because when orthodontic care starts when someone is a child, their jaws have not finished growing. This makes it easier for the specialist to guide the jaw (and other facial bones) into the right positions. Adults often require more surgeries because their bones are fixed. So, for adults to get their desired results, it often takes more surgical intervention.
With surgical orthodontics, cuts are made inside of the mouth. They are not made through the skin. This type of surgery is performed under general anesthesia. It may or may not take place in a hospital. Many oral surgeons have their own facility that is approved to offer these treatments. The bones that are repositioned will be reinforced with titanium. The titanium remains inside of the body. There is usually no need for a second procedure to remove the titanium. Most patients who undergo this type of surgery can still fully use their jaw directly after the surgery. They will suffer from some discomfort and soreness and are often advised to stick to a diet of soft foods. It can take up to six weeks to fully recovery from oral surgery of this nature.
Finally, in many instances you will use braces to reinforce the position of the teeth. In some instances, treatment ends after the surgery.
 What Is Craniofacial Orthodontics?
What Is Craniofacial Orthodontics?
Craniofacial orthodontics is a specialized area of orthodontics that focuses on treating cleft lips and palates, as well as other birth defects that affect the development of the teeth and jaws. Specialists in the field do not work on their own. Rather, they most often partner with other specialists including speech therapists, oral surgeons and plastic surgeons who specialize in craniofacial repairs. Craniofacial orthodontics handles the non-surgical portion of treating cleft lip and palate.
What is Cleft Lip and Palate?
Cleft lips and cleft palates are birth defects. They are facial and oral malformations. The condition develops in utero during an extremely early part of the pregnancy. A cleft signifies that there is not enough tissue in the mouth or around the lip. Therefore, the areas do not join together as they should.
A cleft lip means that the lip is split into two parts instead of being one. It causes a gap to appear between the two parts of the lip. It can even extend beyond the base of the child’s nose. Because of the lack of tissue, the split in the lip can also mean that there is less bone and gum tissue in the mouth. The area behind your upper top teeth is known as your palate. A cleft palate is when there is a split in the palate like in the lip. It can happen at the front of the palate in the bony area or it can occur toward the back of the palate in the softer area.
Cleft lips and palates can be an extremely serious condition. They can affect only one side of the lip and palate or both sides. A cleft palate is the fourth most common birth defect in the United States. It occurs in around 1 of every 700 births.
Clefting is something that is quite obvious at birth. That makes diagnosing a cleft lip and palate easier than other types of birth defects. Often, it can even be diagnosed through ultrasound before the baby is born. This is important because there are times when a cleft lip and palate may be indicators of other abnormalities.
How is Cleft Lip and Palate Treated?
Generally, treatment for cleft lip and palate requires surgical correction. Craniofacial orthodontists specialize in the treatment of this condition. However, it can be rather challenging to estimate the number of surgeries that could be required to correct it. Naturally, treatment depends on the severity of the disorder. The optimal time for treatment of cleft lip and palate is between three and six months of age.
The first surgery is designed to repair the palate. The goal of this surgery is to minimize the likelihood of liquids to develop in the ears. This surgery will also help the child’s jaws and teeth grow into the right places.
Often, children undergo another surgery for cleft lip and palate when they are around 8 years old. The goal of this surgery is to perform a bone graft (although this isn’t always needed). The bone graft supports the permanent teeth and may also be used to fill in the upper gums.
Further surgeries for cleft lip and palate that occur from this point are often done to help the child improve their speech. Generally, future surgeries are only needed by around 1/5 of the children diagnosed with cleft lip and palate.
Sometimes, the additional surgeries do not serve the sole purpose of improving speech only. There are times when future surgeries are needed for functional and/or cosmetic reasons. Some children need surgery to help them improve the way that they are able to open and close their mouths. Or they may need surgery simply to improve the appearance of the skin. In other cases, they may need surgery to help improve breathing.
Can There Be Complications from Cleft Lip and Palate Treatment?
Thankfully, when cleft lips and cleft palates are treated using craniofacial orthodontics at an early enough age, they could very well achieve a normal appearance, giving the patient normal speech patterns and the ability to eat without issues. When children with cleft lips and cleft palates are not treated, serious complications can occur including:
- difficulty feeding as babies
- difficulty eating as they get older
- ear infections as a result of fluid build-up
- hearing loss
- future dental problems
- speech difficulties
- low self-esteem
How is Cleft Lip and Palate Treated?
If your child is born with cleft lip and palate, you should consult with a craniofacial orthodontist. One of the keys to successfully treating clefting is early dental intervention. Your craniofacial orthodontist will show you the proper way to care for your child’s mouth. If your child’s mouth and teeth cannot be properly cleaned with a soft bristled toothbrush, your child’s craniofacial orthodontist can recommend a tool known as a toothette. Your child’s routine dental care (check-ups, cleanings, and fluoride treatment) should begin around their first birthday.
Craniofacial orthodontics should begin before your child’s teeth begin to emerge from the gums. Early surgical intervention usually occurs around three to six months of age. This is crucial for future oral development. The other benefit to early contact with an orthodontist is having an expert who can answer your questions. Your child’s facial development will be assessed and a plan will be made to best treat your child’s cleft lip and/or cleft palate. Additionally, after your child’s permanent teeth have come, the orthodontist can help align the teeth.
Post-care may include speech, plastic surgery and the use of dental appliances to help make up for any missing teeth. Your child may also need a palate lift or a speech bulb. The craniofacial orthodontist will work directly with the speech therapist if your child requires either of these dental appliances to help normalize their speech.
Innovative Orthodontic Appliances
 What Is A Temporary Anchorage Device?
What Is A Temporary Anchorage Device?
TAD is an abbreviation for temporary anchorage devices. In the simplest explanation, TADs are mini-implants in the mouth. The function they serve is to hold the teeth in a certain place. Orthodontists frequently use temporary anchorage devices to align and support the teeth of the patient during treatment.
Temporary Anchorage Devices are relatively new to the market. The FDA only recently approved them for use in 2005. Before TADs, many patients had to use headgear in order to keep their teeth in place. The issue with headgear lies in patient cooperation. If patients do not wear the headgear as directed, their teeth will not fully benefit from orthodontic treatment. TADs enable orthodontists to ensure that the teeth have proper support for the correct amount of time. Currently, TADs are the most reliable method to anchor teeth during the treatment process.
There are two types of TADs: an indirect anchorage and a direct anchorage. An indirect TAD links to your teeth. Orthodontists use TADs when they do not want to anchor the teeth to each other. This is because it is more flexible. A direct TAD is an anchor that supports tension on certain teeth that need to be moved. TADs are removed after the orthodontic treatment is completed.
How Are Temporary Anchorage Devices Placed?
During orthodontic treatment, orthodontists usually have to remove premolars to make room in the mouth to move the teeth into their proper positions. TADs are important because they can help support teeth during the orthodontic process instead of having to remove them. TADs also provide anchorage when the orthodontist must move teeth. They can also help to anchor teeth when there is a need to correct a gap between the teeth.
TADs are made out of titanium alloy. Titanium alloy is extremely strong and doesn’t rust. That’s two of the many reasons why titanium alloy is an ideal choice of material for TADs. TADs have two parts. The first part is the implant head. This is the part of the TAD that is used to secure the teeth. The second part of the TAD is the implant body. It is similar to a screw in nature. It is put into the bone to act as an anchor.
The head of the TAD has an eyelet that is used by the orthodontist to thread the wire through in order to secure the teeth. TADs have a smooth part that both suppresses growth of the gum material where the implant is located and to also minimize the risk of bacterial infection.
There are several different TADs. Your orthodontist will let you know which TAD will best meet the goals of your treatment. Regardless of the type, the screw portion of the TAD is drilled into the jaw. Although it may sound painful, it’s often not. It’s generally painless because the bone in your jaw has no pain receptors. Your orthodontist will first apply a topical analgesic to numb your oral tissue. You will feel pressure when your orthodontist inserts the TADs.
In fact, TADs are also not painful to remove. When it is time for your TAD to be removed, your orthodontist will apply a topical analgesic to numb your oral tissue. Then they will back the TAD out. It usually takes only a few seconds.
Are Temporary Anchorage Devices Painful?
Generally, most patients experience no discomfort after the procedure. If you do find that you have discomfort from your TADs, take some over-the-counter pain reliever such as Tylenol or ibuprofen. If you are experiencing discomfort in the gum line, you can take over-the-counter medication or cover the tip of the TAD with a cotton swab. Then, make an appointment with your orthodontist.
How Do I Keep My Temporary Anchorage Device Clean?
Believe it or not, keeping your TAD clean is extremely easy. You will clean your TAD three times each day using a soft toothbrush. Your orthodontist will also give you a special mouthwash to use. It is important that you use it as directed. The mouthwash helps minimize the growth of microbial bacteria that can cause infection. You should use mouthwash twice each day.
How Long Are Temporary Anchorage Devices Needed?
How long you will need a TAD depends on the problem that your orthodontist is correcting. A patient usually does not require a TAD for longer than a few months. Again, though, this depends largely on your specific issue. Your orthodontist will be able to give you an idea of how long you’ll need the TAD.
 What Are Clear Braces?
What Are Clear Braces?
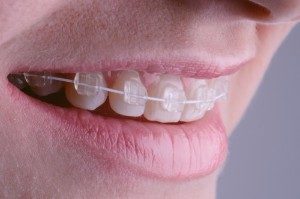
Clear braces, or invisible braces, are less conspicuous than traditional braces. These are ideal for both adolescents and adults. The purpose of clear braces is to not draw attention to the mouth. Hence, they are less obvious. As a result, the wearer is more confident about their appearance whilst undergoing orthodontic treatment.
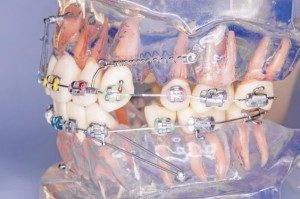
Traditional braces are made from stainless steel. The brackets are cemented onto your teeth. The metal wires, known as a metal archway, is run through the bracket. Clear braces perform the same job as traditional braces. While traditional braces make use of metal wires, or a metal archway, clear braces allow patients to choose between clear ceramic archways or metal ones. Clear archways are preferred by people who struggle with the prospect of sporting unsightly metallic braces.
After the orthodontist affixes the braces to your teeth, you will visit him/her every 4-6 weeks for adjustments. The typical amount of time that one wears clear braces is 1-3 years. After treatment is complete, patients wear retainers to keep their teeth in the right place.
Patients are advised to follow their orthodontists’ instructions about the maintenance of the braces. Not doing so can cause noticeable discoloration of the braces. We advise patients to stay away from consumables that cause staining, like coffee, tea, red wine, tomato-based sauces, curry, and smoking.
It is also important that you brush your teeth three times a day. These are best practices for good oral health, and it will help protect clear braces from staining. Additionally, you should carry on your person a travel toothbrush and a small container of toothpaste the event that you are dining out and discover food stuck in your braces. While the same holds true with metal braces, it becomes distinctly more noticeable with clear braces.
What Is The Difference Between Clear Braces and Clear Aligners?
Clear braces and clear aligners are not the same thing although they serve the same purpose. They both straighten your teeth in a less obvious way than wearing traditional braces or aligners. A series of clear aligners are designed for you based on the goals set by you and your orthodontist to straighten your smile.
Clear aligners can help straighten moderately crooked smiles and can sometimes even be used to correct problems with your bite. Of course, clear braces can be used to treat a wide array of orthodontic issues.
Regardless of your age, if you worry about misplacing items or if you worry that you will forget to wear the aligner, then you may want to consider clear braces. Clear braces are attached to your teeth. So, you don’t have to worry about losing them or forgetting to put them in your mouth. Clear aligners are worn for up to 22 hours each day. You should only remove them when you eat, brush your teeth, or floss.
Clear aligners may require you to have attachments placed on your teeth. Attachments are a build-up of a composite that matches the color of your teeth. They’re like little ridges. They help keep your aligners in place.
Clear braces stay in your mouth while you eat, which is why orthodontists advise avoiding foods that could stain your braces or teeth. Cleaning clear braces is easy. You simply brush your teeth regularly. You don’t necessarily need anything special. With clear aligners, the manufacturer may recommend that you use only their cleaning system. Although you may also be able to remove your clear aligners and brush them with toothpaste and rinse them out, the specialized systems keep bacteria at a minimum.
When it comes to the cost of clear braces and clear aligners, here’s what you need to know. Often, clear braces are a little more expensive than traditional braces. However, your dental insurance company may pick up a portion of the cost. Many people find that the extra expense is worth it since they are less obvious than traditional braces. Clear aligners are also a little more expensive than clear braces. Then, you may also have the added expense of a cleaning system. Your dental insurance policy may not cover the use of clear aligners.
After your orthodontic treatment is completed, you may need a retainer (regardless of whether you used clear braces or clear aligners). Talk with your orthodontist about how many retainers you may need and if that cost was included in your treatment.
What Are The Advantages and Disadvantages of Clear Braces
There are two distinct advantages of clear braces. The first is that clear braces are more favorable aesthetically. The brackets are distinctly less obvious with clear braces. This is because they are made from ceramic. This is a huge benefit for people who feel self-conscious about the fact that they will be pursuing orthodontic treatment. The second advantage is in the treatment time. In many instances, clear braces provide results faster than clear aligners.
There are some disadvantages with clear braces. The first is that some may find the cost restrictive. Clear braces are more expensive than traditional braces. If clear braces are outside your financial reach, talk with your orthodontist about financing options. The second disadvantage is that the ceramic brackets are susceptible to staining. If any staining occurs, the brackets will likely become more conspicuous. Patients usually dedicate considerable time and effort to keep clear braces clean.
Who Are Good Candidates for Clear or Ceramic Braces?
Your orthodontist will likely refer to clear braces as ceramic braces. To determine whether or not clear braces are the right option for you, you need to:
- Make sure that you really can and want to devote the extra time it will take to keep your clear braces clean.
- Make sure that you can devote yourself to giving up certain foods and drinks (and smoking) during your treatment. Not doing so will stain ceramic brackets.
- Check on the cost and check with your dental insurance company. Find out what portion you will be responsible to pay. Talk with your orthodontist to ask about financing options, if needed.
- Consult with your orthodontist about whether clear braces are the best choice for you. Although orthodontists may use clear braces to treat those issues typical of traditional braces, it is important to speak to your orthodontist first. He/she is the only professional who will be able to help you decide which treatment is best for you.
 What Is Invisalign?
What Is Invisalign?
Invisalign® is a system of clear aligners that help teenagers and adults get the straight smiles they want without using traditional or clear braces. Since Invisalign® aligners are made specifically to treat your orthodontic needs, they are often more comfortable for you to wear.
The FDA has classified Invisalign as a Class II medical device. The FDA cleared Invisalign® for use by the public in 1998. Invisalign® aligners and retainers are phthalate free. They are made from Class VI (medical grade) high molecule weight polyurethane resins.
Invisalign is more expensive than traditional braces. However, for a lot of patients, the increased rates are worth it. You should review your dental insurance policy to determine if it covers the cost. Many Invisalign providers also have financial plans to make the smile of your dreams more affordable.
What Are The Benefits of Invisalign?
Invisalign® has many benefits. First, Invisalign is more comfortable than traditional braces. If you currently have traditional or clear braces, you can talk with your orthodontist to find out if you can switch to Invisalign. Many orthodontists treat their patients by combining the use of traditional braces and Invisalign.
One of the things that people hate about having traditional or even clear braces is that they have to give up certain foods during treatment. With Invisalign, there are no food restrictions. One of the few times you remove your aligners is when eating. Then, you clean your teeth and put your aligners back in. You can continue to eat crunchy foods, drink coffee, and eat foods with tomato-based sauces. The only restriction generally given with Invisalign is to avoid chewing gum. This is because chewing-gum sticks to your aligners.
If you’re worried about the pain often associated with using traditional braces, then you should consider Invisalign. Although some patients report minor discomfort in the first few days of a using a new aligner, it is generally far less uncomfortable than traditional or clear braces. Patients often report it not as feeling painful, but as a feeling of pressure in their mouth.
Invisalign is clear and easy to use. It is great for people who are worried about the attention they may get from wearing traditional braces. Since they look and fit similar to a custom whitening tray, they aren’t as noticeable during treatment. Some patients do report having a small lisp during the first few days of treatment. However, this goes away as your tongue learns to navigate in your mouth with the aligners.
Invisalign treatment takes, on average, about a year. However, it could take more time to help you get the smile of your dreams. Invisalign has come a long way since its first approval for use in 1998. Orthodontists now use it to treat various bite problems. So, if you thought you wouldn’t qualify for Invisalign, check with an orthodontist specializing in its use. You may be pleasantly surprised!
How Does Invisalign Work?
First, you should visit with an orthodontist who is trained in the use of Invisalign®. Many offer free consultations. However, when you call to make an appointment, you should ask if they will charge you for this initial appointment. Your orthodontist will assess you and determine if Invisalign is the right choice to help you straighten your smile. He can also talk to you about Invisalign options: standard, teen, or express treatment.
Your orthodontist will take dental impressions of your teeth as well as measure them. Dental impressions may be digital or your orthodontist may do them out of a putty tray. Your orthodontist will also take a bite registration. This helps your orthodontist better understand how your teeth meet. They will also take X-rays to determine the root positioning for your teeth. Finally, the orthodontist will take a series of photos. This will help document the progress of your treatment. At the end of this portion, the office might ask you to make a payment for your treatment. So, you should make sure that you know if your dental insurance will pay for any of the treatment and what your financing options are if you cannot pay in full.
Your orthodontist will send the information about your bite and your teeth, including the photos, to Invisalign. Invisalign will create a digital simulation of the movement your teeth will undergo with treatment. Your orthodontist will review this digital simulation to ensure it is correct. Once approved, Invisalign will make your aligners. How many you will need will depend on the goal of your treatment. Some people just need 10. Others need as many as 30.
Your orthodontist could receive your aligners in as little as 2-3 weeks. However, if the treatment plan requires changes, it could take longer. Once your orthodontist has your retainers, they will contact you to schedule an appointment. The orthodontist may put “attachments” on your teeth. Attachments are a composite material that matches the enamel color of your teeth. They are put on the front of some of your teeth to help keep the aligners in place. You’ll wear each set of aligners for just a few weeks. You’ll visit the orthodontist every four to six weeks to monitor your progress. Invisalign also has a custom cleaning kit for your aligners. Although you can remove your aligners and clean them with a toothbrush, the custom cleaning kit is still important.
At the end of your treatment, you may require the use of retainers in order to keep your teeth in their new place.
 Cutting-Edge Diagnostic Tools and Technologies
Cutting-Edge Diagnostic Tools and Technologies
Dental and orthodontic treatment have come a long way during the last few decades, and not just in treatment options. Before your dentist or orthodontist fills cavities, performs root canals or oral surgery, or even fits you for certain types of oral appliances, they first take x-rays and other imaging of your teeth. This helps your dental professional ensure that they choose the right treatments.
What Is An iCat Scan?
An i-CAT® Scan is used by orthodontists to create a 3D view of your teeth and the craniofacial structure. It takes less than five seconds. i-CAT Scan is revolutionary not just because of its 3D results and quick use. It also helps protect you from being overexposed to radiation. The technology can be specifically targeted and provides a lower dose of radiation than older options.
i-CAT Scan helps ensure that your dental or orthodontic treatment is perfect for you. It gives your dental professional more accuracy and clearer images. If you need a temporary anchorage device, iCAT® Scan makes the placement options perfectly clear to your orthodontist. For younger people, i-CAT Scan can still be used. This technology can help dental professionals assess teeth that have yet to surface as well as showing root placement and impactions.
i-CAT Scan has different options for use depending on whether you need implants or orthodontic care.
Are i-Cat Scans Safe for Pregnant Women?
There are times when pregnant women need dental implants or orthodontic care that may not be able to wait until after the birth of their baby. Although i-CAT Scans have a low radiation exposure, your dental professional may advise you to hold off as long as possible. There are often temporary measures that can be implemented by your dental professional in order for you to get some amount of treatment now if necessary and wait until after the baby is born for an i-CAT Scan.
What Is A CBCT?
A CBCT, also known as cone beam computed tomography is another recent advancement in dental technology. It provides another quick way for dental professionals to examine the positioning of your teeth, their roots, and the bones in your face. It takes only 20 seconds and, much like an i-CAT Scan, it has a much lower dose of radiation than older types of CT scans. This type of scan is used to help plan your dental treatment.
Common uses for CBCT include planning for dental implants, oral and maxillofacial surgery, orthodontic treatment, and the assessment and treatment of TMJ.
Is CBCT Dental Imaging Safe for Pregnant Women?
Because a CBCT dental imaging procedure is a CT scan, we do not recommend it for pregnant women. There is no known “safe” level of exposure for unborn babies. This is why it is safest to wait for this type of dental scan until after the end of your pregnancy.
What Should Patients Know About CBCT?
Because the i-CAT® Scan and CBCT imaging are both a form of CT scan, there are somethings that you need to know. As mentioned earlier, both have a lower amount of radiation exposure than their predecessors. Regardless of which of these scans you will undergo, the things you need to know are the same.
The processes are painless. You sit upright in a chair. In most CBCT dental imaging, a device moves around your head. It takes a lot of pictures in a very short amount of time. Because both the i-CAT Scan and CBCT Dental Imaging Machines take the pictures so quickly, it is ideal for both younger patients and older patients. For your dental professional to get the best images possible from the i-CAT Scan or a CBCT Dental Imaging Machine, you must sit still. This keeps the images from being fuzzy.
Wear comfortable clothing. You should not wear jewelry including earrings, necklaces, or piercings. Ideally, you should not wear hairpins or glasses. You may be asked to remove any dental appliances that are in your mouth. This may include your dentures. However, do not just leave your dentures or dental appliances at home. Your orthodontist may find them useful after the scans in order to help plan your treatment.
You should reach out to your dental insurance company, or call our office before your scan. It’s important that you know if any portion of the i-CAT Scan or CBCT dental imaging is covered. If so, what portion of the payment you will be responsible in covering.
Complications That Can Arise If Orthodontic Issues Go Untreated
 What Is Sleep Apnea?
What Is Sleep Apnea?
Sleep apnea is a condition that causes people to either stop breathing or their breaths become extremely shallow during sleep. Sleep apnea affects 22 million Americans. These shallow breaths or the lack of breathing can last seconds or minutes. Normal breathing often restarts with a choking or snoring noise. Sleep apnea can cause you to feel unrested even if you slept for seven hours or more. This is because the symptoms of sleep apnea often causes patients to leave their deep sleep and enter into a lighter sleep.
What Are Some Signs Of Sleep Apnea?
There are some common signs of sleep apnea. Some you may notice and some you may not notice in yourself.
- Unusually loud snoring.
- You stop breathing during your sleep. This is a sign that somebody else will usually notice first.
- You wake up suddenly feeling short of breath.
- You wake up with an unusually dry mouth or with a sore throat.
- You wake up every morning with a headache.
- You struggle to fall asleep or stay asleep (or you struggle with both).
- You are excessively tired during the day.
- You struggle to pay attention during the day.
- You’re irritable.
If you have these signs or if someone in your family tells you that they’ve noticed them in you, you should make an appointment with an experienced orthodontist to talk about your concerns.
Are There Different Types Of Sleep Apnea?
There are three different types of sleep apnea. The first type is obstructive sleep apnea (OSA). It is the most commonly diagnosed type of sleep apnea. Studies suggest that only about 10% of people with OSA receive medical treatment. This is because the majority of OSA sufferers are often undiagnosed. Obstructive sleep apnea occurs when part or all of the airway is blocked during sleep. This may happen because the tongue rolls toward the back of the mouth or because a patient has an excess of fatty tissue that blocks the throat. OSA diagnoses range from mild, moderate, or severe.
Mild OSA means that the sufferer experiences between 5 and 14 interruptions each hour during their sleep cycle.
Moderate OSA means that the sufferer experiences 15 to 30 interruptions each hour during their sleep cycle.
Severe OSA means that the sufferer experiences 30 or more interruptions each hour during their sleep cycle.
Central sleep apnea (CSA) isn’t caused by your airway getting blocked by your tongue or other fatty tissue. Instead, central sleep apnea occurs when your brain doesn’t send the message to your muscles to keep breathing. Your brain is part of your central nervous symptom. Your brain isn’t communicating properly to keep you breathing normally when you’re asleep. CSA isn’t as common as OSA. It is a side effect of a brain injury or a medical issue that affects the brain. With CSA, a common symptom is mood swings.
The third type of sleep apnea is complex sleep apnea. This means that you have a combination of OSA and CSA. Healthcare professionals will usually diagnose complex sleep apnea after a sleep study that shows a patient has signs of each.
What Are The Risk Factors For Sleep Apnea?
Risk factors vary depending on the type of sleep apnea. However, some factors are common with all three types.
Risk factors for OSA include:
- Being overweight. This can cause an increase in fatty tissue that restricts the flow of air as you sleep.
- Your age. As we get older, we lose muscle tone even in our throats. Since the muscles are weaker, they can collapse over the airway and make it harder to breathe when you are sleeping.
- Enlarged tonsils or adenoids. These can block your airway.
- Frequent use of intoxicants. This can cause the throat muscles to relax and block the airway during sleep.
- Smoking can cause irritation to your airway and make it harder to breathe.
- Family history. Genetics play a major role in the development of sleep apnea. Those with a family history of sleep apnea are at an increased risk.
Risk factors for CSA include:
- Parkinson’s Disease.
- Brain infection.
- Use of narcotics.
- Heart failure.
- Being overweight.
- Atrial fibrillation.
- Sleeping at higher altitudes.
- Brain tumor.
- Use of opioid medication.
It is important to note that complex sleep apnea includes the risk factors of both OSA and CSA.
Is Sleep Apnea Dangerous?
Sleep apnea can be dangerous. It deprives our bodies of the oxygen we need to function properly. When this happens, we suffer more than a poor night’s sleep or fatigue during the day. Untreated, sleep apnea can cause numerous health problems. Sometimes, the symptoms of sleep apnea are signs of an underlying health condition.
Untreated sleep apnea can lead to high blood pressure. For people who develop high blood pressure because of sleep apnea, the former usually gets better once they start treatment for the latter. It can also lead to heart disease and heart attacks. This is attributed to the heart getting the oxygen that it needs and from the stress of not sleeping.
Another complication of untreated sleep apnea is diabetes. Although there’s not a direct link between the two at this time, the common symptom of obesity is a link between the two diseases. Many healthcare professionals believe that lack of sleep can cause you to become insulin resistant. Insulin resistance is a warning sign of the onset of diabetes in the future.
Sleep apnea can cause or exacerbate many mental health problems. The lack of sleep can cause you to develop symptoms of anxiety and depression. It can also cause current mental illnesses to become more pronounced.
How Is Sleep Apnea Treated?
How sleep apnea is treated depends, ultimately, on which form of sleep apnea you are diagnosed with. OSA has several treatments. Some treatments are more conservative than others. It may be treated by use of a CPAP, an APAP, or a BIPAP machine. These machines force air through your airway while you are sleeping. This is known as positive airway pressure (PAP). Your doctor may prescribe the use of an oral appliance. An oral appliance is something that a patient wears in their mouth while they sleep. The two main types hold your jaws in a certain position and hold your tongue in a certain position. The objective of both is to keep your airway from becoming blocked. For severe OSA, surgery may also be an option.
Central sleep apnea is often treated with a CPAP or BPAP. Another option is an ASV. An ASV is an Adaptive-servo ventilation device. It makes automatic adjustments to compensate for any abnormal breathing patterns the patient may have when they are asleep. Medications may also be prescribed to people who have CSA. Usually, medications are not prescribed unless positive airway pressure doesn’t work.
Complex sleep apnea treatments will ultimately depend on which symptoms you exhibit. We can help develop a custom plan to treat your CSA.
If you believe that someone in your family has sleep apnea, you should keep a list of the symptoms and when they occur. Then, talk to the person about the benefits of being evaluated for sleep apnea.
 What Is TMJ?
What Is TMJ?
Temporomandibular joint disorder is often abbreviated and referred to as TMJ or TMD. In fact, you may find that many dental and healthcare professionals use the terms TMJ and TMD interchangeably. The joints involved in this disorder are located on each side of your head. The joints work with the muscles and ligaments to help you open and close your mouth for talking, chewing, or yawning. TMJ / TMD happens if these joints do not work as they should.
Despite the location of the joints involved, TMJ / TMD can affect face (and your head) in other locations. TMJ / TMD causes chronic facial pain. It is most commonly diagnosed in people between the ages of 20 and 40 years old. According to the American Dental Association, this condition is more common in women than in men.
With TMJ / TMD, the joints of your jaw do not work in the way that they are designed. Treatment does exist for TMJ / TMD. Generally, the goal of treatment is to control or stop the symptoms of the disorder. Treatment could include finding a way to minimize the spasms that occur in the muscles and the ligaments around the affected joints. Sometimes, dental professionals prescribe the use of specialized dental appliances to help reduce the likelihood of negative problems that result from the disorder. Relaxation techniques are often taught in order to help the patient learn how to lessen the tension in the jaw muscles. In extreme cases of TMJ / TMD, surgery may be recommended.
What Are The Symptoms Of TMJ?
TMJ / TMD is often symptomatic. Yet, one issue with relying only the symptoms is that there are other dental and craniofacial issues that have similar symptoms. It is very important that if you see any of the following symptoms that you see a dental professional. Your dentist will take a complete history of your dental and physical health. Then, you’ll most likely undergo x-rays so that the dentist can examine the jaw bones and teeth. The dentist will also perform an exam.
Symptoms of TMJ include:
- Severe headaches. Many patients with TMJ believe that they have a migraine because of the location and severity of the pain.
- Because of the close proximity of the jaws to the ears, when patients have TMJ, they often experience earaches. It could be dull pain or sharp pain.
- Clicking or popping when you open or close your mouth. Additionally, the jaw may also lock into place. Although no one knows what causes TMJ, many theorize that it is a form of arthritis in the jaw.
- Pain or tenderness in the jaws. Inflammation in muscles and ligaments can cause pain. Grinding of the teeth can also cause pain.
- Your upper and lower teeth do not fit together anymore. If your bite was normal and suddenly becomes abnormal, you may have TMJ.
If you have certain risk factors, it is more likely that you will develop TMJ / TMD. Risk factors include a diagnosis of certain types of arthritis, experienced an injury to your jaw, have a history of grinding or clenching your teeth, or have certain connective tissue disorders.
If TMJ / TMD is left untreated, complications may develop. Common complications related to this dental problem include poor oral health, long-term headaches, sleep loss because of grinding of the teeth, malnutrition, eating disorders, and hearing problems. If you have suspect that you may have TMJ / TMD, see a dentist right away.
Is All Jaw Pain Associated With TMD?
Not all jaw pain is associated with TMD. While TMD occurs in around 10-15% of the population, other conditions have similar symptoms. These include:
- Sinus infections. Sinus infections can be really mild and have practically no symptoms passed pressure in the sinuses or they can be severe. Severe sinus infections can do more than cause pressure in the face. It can cause ear pain, dizziness, and some people even experience jaw pain.
- Problems with neck muscles. As you learned earlier, jaw muscles can cause ear pain. Neck muscles can cause jaw and ear pain. Our muscles in the craniofacial region are interconnected. So, you may not have TMD, but you could have a pulled or strained muscle in your neck and shoulder region that is causing you pain in your jaw and ears.
- An abscess. If you have an abscessed tooth, it can eventually cause jaw and ear pain. Signs of an abscess, aside from pain, includes a swelling of the face, a buildup of pus under the gum line, a blister like sore on the gum, or even a fever. An abscess requires treatment with antibiotics or it can become life threatening.
- Bruxism means that you spend a lot of time grinding or clenching your teeth. It’s likely that you don’t do it on purpose. It is something that you can do in your sleep. The result is often pain in the jaw.
- Trigeminal Neuralgia. Trigeminal neuralgia is the inflammation of the trigeminal nerve. This particular nerve gives feelings to your mouth. It can be moderate in nature and only cause minor pain when eating or it can be so severe that the face begins to ache from a soft breeze.
 Frequently Asked Questions
Frequently Asked Questions
What is the difference between an orthodontist and a general dentist?
An orthodontist is a dentist first. Firstly, they graduate from dental school. Following this, they go on to specialize in orthodontics. This is typically a 2-3 year residency program that follows dental school.
Do I need a referral to see an orthodontist?
Very often, new and potential patients ask if they need a referral from their general dentist. The answer is no. Anybody can call and make an appointment for an initial consultation. In fact, we encourage them to do so.
Because we do not charge a fee for initial consultations, it is a good idea to come into the office and learn what might need to be done in the future.
To conclude, you do not need a referral from your general dentist.
How does orthodontic treatment work?
Meetings with patients and their parents, often include the question, “How does orthodontic treatment work?” The answer depends on each patient’s specific situation and the type of treatment needed.
The first step for some patients is to create space for the teeth to be made straight which often includes expansion. This is so we have the space we need when the time comes to put braces on or use Invisalign.
For adults, treatment may be a tad different because we do not have the same options when it comes to creating space. However, as far as how orthodontics work in general, it basically creates space through expansion or other means. Following this, we use braces, Invisalign, or other modalities to make the teeth straight.
The last aspect is just making sure the upper and lower jaws fit together as they should.
Does insurance cover orthodontic treatment?
Insurance that covers orthodontics has become very important in the past few years. As a practice, most clinics try to identify most of the big insurers in the area and partner with them.
This is important because of the fact that patients benefit most when they work with a participating provider. As a result, they may take advantage of lower fees that providers negotiate for members thereby reducing patient costs.
This also means that payments go directly to the orthodontist, which can reduce patients’ out-of-pocket expense. Needless to say, but that is incredibly important for families to know.
If patients choose an out-of-network provider, they will first need to pay the full amount. The insurance provider will then reimburse them. However, these patients miss out on availing of the discounts available to those working with a participating provider.
OrthoWNY participates with nearly all of the major insurers in the area. in addition, we also make an effort to identify these insurers in all of the communities where we practice.
What is the average cost of orthodontics?
This question is hard to answer without seeing and examining a patient. This is due to the fact that orthodontic fees are based on the degree of difficulty. Hence, the more difficult the case, the higher the cost.
We sometimes plan treatment in stages that we call phases, and the fees may be lower for certain aspects of treatment.
The best way to determine your specific cost is to visit our office and let us give you a detailed picture of what the costs will be. This will include how insurance plays into it and what your total out-of-pocket costs will be.
How long does orthodontic treatment take to complete?
Every case is individual and unique. That is why we offer free consultations. When a patient comes in for a first consultation, we examine their problems. We then explain to the patient what is wrong, what needs work.
Once patients recognize the extent of the problem, it becomes simple for them to understand how we estimate the length of their treatment.
Some treatments can be completed in as few as 12 weeks, while others may take two years. In some cases, it may even take longer. The average orthodontic treatment, across the profession in general, is approximately 24 months, even though many cases can be treated in less time.
What are the goals and objectives of orthodontics?
Orthodontics has, as its ideal goals and objectives, the achievement of a perfect bite. A perfect bite is one in which there is a functional relationship between the upper and lower jaw, and where the teeth are staggered between one another, intercuspating, or fitting together like the teeth between gears. With that relationship, orthodontists hope to achieve optimal functional stability for the patient’s teeth and musculature.
Orthodontic treatment’s added benefits include creating foundations for future dental work. Therefore, this enables the restorative dentist to create their best work.
By achieving these ideal goals and objectives, we seek to achieve functional stability in the musculature and the functions that occur inside the oral cavity – whether they involve breathing or swallowing.
Orthodontic treatment goes beyond the treatment of teeth to include the side benefit of enhanced aesthetics. However, most patients actually seek our care to improve aesthetics. But in reality, our treatments are geared more toward the functional aspects. Aesthetics are a byproduct of what we accomplish by achieving those other goals.
When is the best age to visit an orthodontist?
The American Association of Orthodontists recommends patients be screened as early as age seven. Doing so enables us to identify contributing problems that might require additional orthodontics in the future.
Not every patient who comes into the orthodontist’s office at age seven starts treatment. However, it is wise to have an educated eye examine the patient to identify factors that may contribute to a need for intervention and begin making corrections. A more profound impact is possible with a younger patient than with an older one.
Age should not be the only determinant, however. If a parent suspects a problem in their child who is younger than seven, or if the child’s general dentist recognizes a problem and wants to make a referral, it is never too early to visit the orthodontist for a conversation.
Many times, orthodontists are the first line of defense in identifying other overlooked problems. These include issues like tongue dysfunction, breathing problems, and others. Since it is important to treat those things, a patient can come into our office for an evaluation at any age.
Why is the first orthodontic consultation important?
The patient’s first visit is the most important one. This is because an untreated mouth offers the best opportunity to identify factors contributing to the patient’s orthodontic problems. If we focus only on how we will treat a malocclusion, we may miss the reasons the patient’s teeth are like that in the first place.
We try to be very, very cognizant of the overall condition of patient’s mouth. If we’re not perceptive before starting treatment, the patient’s mouth becomes an altered environment. In such a situation, it may no longer be possible to identify preexisting problems.
We feel that an individualized treatment plan is the most important thing we offer. And it starts with the first visit. This is when we carefully evaluate things that are going on in that patient’s mouth that contribute to their need for orthodontic intervention.
What orthodontic issues need to be seen early?
Certain problems, such as the relationship between the upper and lower jaws, can benefit from early orthodontic treatment.
The upper jaw behaves like a door frame that accepts a door closing into it. A small upper jaw might affect the way the lower jaw is able to close into it. A patient with such a jaw might develop a crossbite. A unilateral crossbite is one problem we prefer to see prior to age seven. It is treated with a simple appliance that corrects the width of the upper jaw while allowing the lower jaw to recenter itself. It, therefore, contributes to more favorable future growth.
Other patients we like to see early on include those who show signs of tongue dysfunction. Or patients who may have developed certain detrimental habits. Sometimes, an orthodontist can talk with these patients and help them to stop a finger habit, for example. If we recognize a tongue pattern problem and cannot treat it ourselves, we may refer the parent to someone who can help.
Very often, tongue dysfunction that is not contributing to an educational deficiency is overlooked because a school’s speech pathologist may not want to identify a tongue thrust.
We feel that regardless of age, if a parent suspects something is wrong, it is a good age to bring the patient in. Allow us to make a critical evaluation of anything that might contribute to a poor oral environment.
What orthodontic problems should I look for in my child?
Parents frequently want to know what signs they should be looking for in their children that might require orthodontic treatment. They want to know what signs precipitate the need for an orthodontist visit. We respond by describing growth and development aspects of orthodontics at a younger age. We further explain to them why those issues are important to treat.
Discrepancies in growth and development may exist in the respective widths of the child’s upper and lower jaws. Ideally, the upper jaw should be biting on the outside of the lower, rather like a doorframe fits a door.
If the “doorframe” is too narrow, the upper jaw will bite on the inside of the lower jaw. In such a case, it becomes very important to begin orthodontics at a younger age. Orthodontists recommend ages between six and eight, which is when widening the upper jaw is very easy.
Another concern is a big overjet. An overjet is when the upper and lower central incisors overlap. Starting treatment early gives us the time needed to help the lower jaw grow forward or push the upper jaw back into a better position.
An underbite should be seen as early as possible too. Because of the genetic component, if the parents have an underbite, we often see them on the children also. Identifying an underbite early is important because our only way of fixing it is to bring the upper jaw forward and help it grow forward. We lose that option once the patient hits the 12-13 year old mark. Therefore, we prefer to see these children young thereby taking advantage of the ability to bring the upper jaw into the proper position.
Also, check for crowding of teeth by looking at your child’s upper and lower front teeth. If there is crowding in the upper and lower front adult teeth, it is likely to increase as more teeth try to come in.
Identifying these early and visiting an orthodontist at a young age allows us to start any expansion that may be required to create more space.
Is there a maximum age for orthodontic treatment?
People of advanced ages have come into my office. Our feeling is that there is no age that precludes a patient from considering orthodontic treatment.
We have treated patients well into their 90s. Although orthodontic in nature, these treatments may not be as comprehensive as those performed on younger patients.
Many elderly patients come into our practice and tell us, “I’ve been wanting to do orthodontics my entire life and I never got around to it. I wanted to just come in here and see if I was still able to have it.”
Treating these patients is very rewarding. This is because of the joy in their lives and in their faces when we are finished. All because of what we have done for them.
What are the phases of orthodontic treatment?
When parents bring their children to us for orthodontic treatment, we recommend a Phase one orthodontic treatment. Such a treatment corrects problems in the structural relationships between the upper and lower jaws. It also tries to correct dysfunctions that might contribute to the malocclusion, or poorly-fitting teeth.
Once we’ve stabilized those structures and functional relationships, we take a break in orthodontic treatment. During this time, the orthodontist monitors the patient to ensure that the treatment is stable.
This interim time can be even more important than actual orthodontic treatment. This is when we watch for changes or reversion that can indicate underlying problems that need treatment.
A rest phase also offers the opportunity to pay very close attention to monitoring the patient’s growth and development, checking periodically to see whether the remaining permanent teeth are erupting into favorable positions.
Many patients who go through phase one orthodontic treatment require very limited orthodontics in the second phase. The second phase is the process of detailing or finishing the job started during the first phase.
We do not have complete control over the eruption of the permanent teeth, which may come into place with minor irregularities. So we recommend correction to improve aesthetics and alignment, and to improve or finalize the structural relationship between the upper and lower jaws.
What is a proper bite alignment?
One of the first things we do with new patients is to tell them exactly how a bite should fit. That way, we can compare their situation to the ideal, which is our objective for every patient. We show the patient how a bite should fit together so that they understand what is wrong with their bite.
Ideally, the upper jaw accepts the lower jaw like a doorframe accepts a door. Additionally, the upper teeth should bite down on the outside of the lower teeth. When biting all the way down, the full length of the lower front teeth should be visible. Furthermore, you shouldn’t bite too deeply over the lower front teeth or have an opening in the front.
The way the bite fits together on the sides is the foundation of our bite. Just like the foundation of a house, it is the most important part of the bite. Even though it is the part nobody sees in the mirror when they smile. The front cusp of the upper molar should fit into the groove of the lower molar so that all the teeth fit together like bricks in a wall.
The most important relationship between the teeth is the fit of the upper canine tooth between the lower canine and the lower first premolar. This is because when you shift your jaw from side to side as you chew your food, and when you clench or grind at night, you glide off of those teeth and help protect your jaw joint. Not only does the fit matter for aesthetic reasons, but they are also important from a functional point of view.
When we compare our family members with ourselves as we try to figure out what might be going on, we can see certain recurring traits.
If the upper jaw is biting on the inside of the lower jaw, we call it a posterior crossbite. We might also see something called an overjet. This is when the upper jaw overlaps the lower jaw, and leaves a gap. An underbite, on the other hand, is when it is in the opposite direction. We may see crowding if the front teeth do not have enough space to be straight.
What are invisible braces?
There are different types of invisible braces. There are those with tooth-colored brackets that perform the same function as metal brackets. The difference is that they are made of ceramic. Therefore, they practically blends in with the teeth.
Options like Invisalign use clear trays that fit over the teeth. These are the modalities we identify most with invisible braces.
The primary benefit for patients – especially late teens and adults – is that these braces are much less noticeable. This helps patients feel better about their appearances because people do not notice their braces as much.
How does Invisalign work?
Most patients who come in for a consultation ask if they can be treated with Invisalign. However, they do not quite understand how Invisalign actually works. The first step is to take a digital scan of the patient’s mouth using a wand. This creates a 3-dimensional representation of the mouth and teeth of that patient.
The first representation is sent to the Invisalign headquarters. There, a technician resets all of the teeth utilizing computer software. The case is then sent back to us. Following this, we evaluate whether or not the technician moved the teeth properly.
Using our software, we fine-tune what the technician did in an attempt to improve upon the result they achieved.
This process is repeated several times. Once we have finalized and accepted our treatment plan, we move on to next steps.
Once accepted, Invisalign will print the retainers using a 3-D printer. This printer actually prints those plastic trays. A patient contemplating a one-year treatment will need 26 sets of retainers to be printed out. This includes both top and bottom jaws. Those retainers are shipped to our office to be dispensed to the patient through the course of the treatment. We may stretch appointments out, giving patients 4-6 sets of retainers and asking them to wear each set for 10-14 days.
Does Invisalign cost more than regular braces?
The answer really depends on that patient’s individual treatment regime. This is because Invisalign treatment is different for different patients. The cost depends on the difficulty of the case, how many trays the patient will require and whether rubber bands will be required.
Each situation presents a different degree of difficulty and results in different fees. Therefore, the best way to be sure is for the patient to come in and discuss the treatment time and costs involved with their case.
Who are the best candidates for Invisalign?
More than ever before, many situations are treatable with Invisalign. So our short answer is that you should let an orthodontist evaluate you for Invisalign.
We can look at the way a patient’s bite fits together and see whether something may be going on that requires treatment before starting with Invisalign. Moreover, we can use Invisalign to address difficult treatments, more now than ever before.
Will my voice change when I am using Invisalign?
Sometimes, the main concern of a patient considering Invisalign is whether they will sound funny when they speak while the trays are in place.
To put their minds at ease, we suggest that patients do a test when they first get their Invisalign. I say, “Talk to somebody who can’t see you. Then, ask them if they thought you sounded funny.”
9 times out of 10, other people will not even be able to tell. Also, the tongue is very tactilely sensitive. And it is quick to detect the slight added thickness of the tray on the backside of the upper front teeth. As a result, patients sometimes feel as though they are lisping – which they may do for the first day or two. However, this tends to go away very quickly.
Do braces go on every child at an early age?
The answer is no. Very often, we start by trying to create room for teeth to be made straight and make the jaws the proper size and shape.
We frequently start with an expander to make more room in the mouth and widen the jaws to the proper width. Then, we go into braces.
Sometimes we do a “partial treatment” using just upper and lower front braces for a short time to align things into their proper positions and attain a proper fit between the upper and the lower. Then, we give kids a long break and wait for the rest of the adult teeth to come in.
Our approach depends on the patient. Sometimes we just do expansion at a young age and sometimes we do expansion with partial braces.
Do braces hurt?
No. Braces are not painful. The forces braces apply to the teeth, however, may cause discomfort.
There is usually no pain associated with the placement of braces. We place wires onto those braces which begin to move the teeth. These wires can cause some discomfort. However, that does not happen immediately. It usually occurs the following day and dissipates soon thereafter.
In the past, patients who had braces put on would suffer discomfort for weeks on end. However, a patient who initiates orthodontics now usually experiences some discomfort on the second and third days after the braces are put on only. Beyond that, their teeth will not be sore at all.
It is important to monitor this in treatment because, if pain persists beyond the first few days, it may be caused by something the orthodontist should address, such as ineffective rubber band wear or wires that may not be doing just what the orthodontist were designed to do. Persistent pain in orthodontics is not a good sign.
Do braces interfere with playing sports and musical instruments?
Younger patients are sometimes concerned that braces will affect either sports in which they participate or musical instruments they play, but we rarely have issues with this. Also, we adapt the mouthpieces required by some sports to fit around any orthodontic appliance we construct. We do encourage our athletes to wear a mouth guard to protect their mouths and to protect against concussions. But we rarely hear of any such issues when they wear a well-fitting athletic mouth guard that’s made for orthodontics.
Musical instruments, particularly brass instruments such as trumpets, trombones and the like, may cause minor irritation on the inside of the lips, making them a little sore. Patients get used to it after a short adjustment period and do not have lasting issues. We have had patients play every contact sport imaginable, with any appliance that we construct in this office. Hence, we feel confident that sports will not interfere with the timing of orthodontics, nor do they adversely affect the decision as to whether or not a patient should have orthodontics.
In our minds, orthodontics is not a barrier to sports and playing musical instruments, nor is participation in either a barrier to orthodontics.
What are expanders? Why are they used?
When a patient has a narrow upper jaw, we first determine if the narrowness is in their jaw or teeth. If the patient has a narrow jaw, we use an expander on the maxillary jaw. Incidentally, the maxillary jaw is comprised of two halves.
Studies conducted at University of Pennsylvania show that patients with a width discrepancy larger than 7 mm between either jaw have a 75% probability of having middle-aged periodontal disease. So it is important to treat any skeletal discrepancy or narrowness in the jaws.
In other cases, the patient’s teeth are narrow. Therefore, we use different types of expanders to move the teeth into a wider position. When we use expansion, we work a little more slowly, and the procedure takes more time.
Some patients may have both narrow jaws and narrow teeth. Such patients will actually be treated with both types of expanders. Instead of trying to accomplish good results using one expander.
We select the appropriate expander for each patient by first taking a radiograph of the front of the patient’s head and physically measuring the width of the jaws in comparison to the width of the head. Next, we measure the width of the teeth in comparison to the width of the jaws and compare the results with standard values that tell us which expanders are appropriate.
Do expanders hurt?
There might be a little discomfort the first couple of days, as you get to used to the little bit of pressure that they put on your teeth, but I wouldn’t call it painful. We always recommend that patients take a little Tylenol or Advil and reassure them that, after the second day, it really gets very easy.
Are expanders removable?
We typically use expanders in our office that we glue onto the six-year-old adult molars. Because doing so makes us sure they will work very efficiently.
Our method allows us to have full control over the situation. In addition, it makes sure we can get the needed width.
We use removable expanders sometimes for specific reasons. However, most often, we use expanders that we glue into the mouth and they work very efficiently.
Why do I have to wear a retainer?
When orthodontic treatment is complete, patients are given retainers. This is because when braces are first removed, the teeth are very mobile. The bone around them has not healed enough to make them more stable. Thus, retainers are necessary to help maintain the orthodontic result.
We typically ask patients to wear retainers at night until their wisdom teeth have been removed. Then, patients are to wear their retainers enough to maintain their fit. Some patients may even need to merely try them on weekly, while others need to wear them as often as every night.
Because patients who are careless in wearing their retainers will experience change – and their parents get upset with them because of their investment – we follow every patient with retainers for at least 18 months. This also depends upon the age at which the patient finished their orthodontic treatment. We will typically monitor patients until we recommend the removal of the wisdom teeth.
How long do I have to wear a retainer after braces?
As each patient gets their braces off, we provide very detailed instructions regarding how the retainers should be worn.
When we remove the braces from teenagers or adolescents, we instruct them to wear their retainers about full-time for 6-8 weeks after the braces come off. Following this initial period, we recommend they slowly reduce their wear to bedtime only. We insist upon patients wearing their retainers to bed. Or at least, until we are certain that the wisdom teeth will not cause changes in the bite.
Once the wisdom teeth are removed – if that is in fact necessary – we instruct patients to wear their retainers enough to ensure that they continue to fit. If that retainer fits right and is not too tight, we can be sure the teeth are not shifting.
Download Our Free Orthodontic Care Guide
Dental eBooks Created and Published by Accelerate Dental Marketing